As many of you may have noticed with the endless facebook posts of Elephants, I had the weekend off and was able to spend every minute of it doing some incredible things. I took a brief two hour flight to Nairobi, obtained my Visa at the airport, was certain to have evidence of my yellow fever vaccine as Ethiopia is high risk and this is needed for entry. I then enjoyed the heck out of an abridged safari through Amboseli National Reserve (about three hours outside of Nairobi depending on how traffic behaves) with some incredible views of Mount Kilimanjaro as well as a variety of wildlife, including my favorite, ELEPHANTS! Our Safari Jeep got stuck in some mud and we had to be towed out by park rangers..but I enjoyed the adventure, Hakuna Matata! But as most weekends do it ended with being back at work Monday morning with so many stories to share.
We had a fantastic morning with a few new patients that came over the weekend with some interesting yet sad stories to tell. Rounds are the act of seeing patients with the team of doctors managing them. This includes the residents(physicians training in Internal Medicine), the fellows (who are training to be Pulmonary/Critical Care physicians)and then me. Each resident carries a patient and that patient is presented on rounds every morning. The presentation is when the resident details the patient's history, physical, laboratory values and imaging as well as formulates a plan to address the pertinent problems with a goal of advancing the patient one more step towards recovery if possible. Each presentation today had an added portion to it---the Ultrasound Exam! What a feeling of pride I had today hearing the residents discuss their Ultrasound findings, an extra step they took with the guidance of the fellows, to use their newly acquired skills to help manage their patients. This has led to the diagnosis of a blood clot in a large vein in the leg of one patient, has helped identify why a patient's oxygen level is low and then was acutely helpful in a scenario in which the lack of certainty with oxygen delivery was again highlighted!
After morning rounds some of the fellows very kindly took me for a traditional Ethiopian lunch. The
dish you see below is a very classic one, injera (the wrap like carb that is the base) topped with several variations of chick-pea based items and some vegetables. You use the excess injera on the outer portion of this dish as your "spoon" using it to sop up the various deliciousness seen below. I can tell you this gesture means so much for them to treat me and their generosity and kindness is so appreciated. We ended our meal with a fragrant cup of coffee and returned back to the hospital.

As we were returning from lunch one of the fellows received a distress call from the residents who are the bedside of a patient who just this morning I had shown one of the first year fellows how to place an ultrasound-guided Intravenous line, one that goes into a central vein (the internal jugular vein in the neck), called a central venous catheter. One of the complications of this catheter placement is that you are potentially close enough to the lung to cause a nick in the lung and collapse of the lung which we call a pneumothorax. Upon arrival to the bedside the patient's oxygen levels (called the saturation) were low and she was hypoxic to 50% (normal saturation is 98%), the fellow quickly looked with the ultrasound for a sign that helps us rule OUT a pneumothorax, she breathes a sigh of relief as this was her first successful placement of such a catheter and to have a procedure related complication would have been very upsetting for everyone. So now we start trouble shooting. Earlier in the day we had noticed that the patient has a lot of fluid in her lungs so we treated this with a medication called a diuretic to help her urinate so she can rid her body of excess fluid. Meanwhile we checked to see if she had a lot of mucous in the breathing tube--nope she did not. We thought about blood clots in the lung as well.
We used something called a Bag-Mask-Valve or Ambu-Bag, which is when we remove the patient from the ventilator and use this device you see here (which is attached to a different oxygen tank) and in using this manually her oxygen saturation increased very quickly. We attached her back to the ventilator and again her oxygenation saturation dropped rapidly.

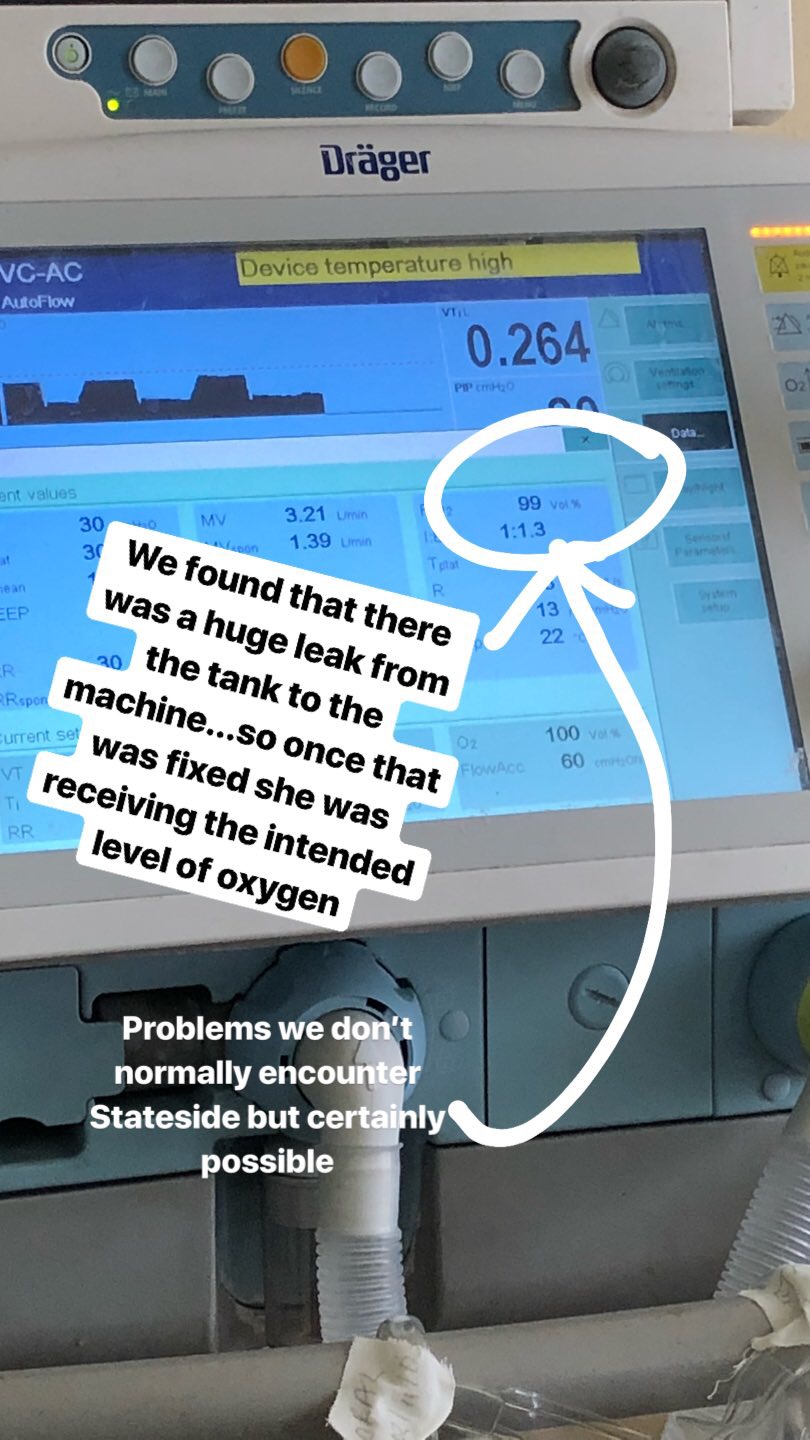
The machine was reading 21% oxygen (room air is made up of about 21% oxygen), however we had set the machine to give her 100% inspired oxygen. What in the heck?! This is when it struck me. THE OXYGEN! there must be a leak somewhere. We checked the tubing there were no holes, we immediately called for someone to help us change the tanks, continuously using the Ambu-bag to maintain her saturation level.

Once the new tank was connected the machine read 99% showing us that now the intended level of oxygen for her to receive was indeed what the machine was sensing and her oxygen saturation remained at an adequate level.
Another day of being kept on my toes, another day of realizing how incredibly gratifying it is to see that our daily practice with the use of the ultrasound is now becoming part of their repertoire, and it is MAKING A DIFFERENCE. Being a teacher comes in all shapes and sizes in all professions--it's part of taking a skill and knowledge that you spent your life learning and sharing it with others for the greater good.
No comments:
Post a Comment